I did not start this piece as a skeptic. I started it as someone who likes numbers, typed “TRT results timeline” into a search bar, and found five almost-identical charts. Week one: energy returns. Week two: fog lifts. Week four: new man. Week twelve: apparently reborn. None of them cited a source I could check. So I pulled the trials myself and ran the numbers against the chart. Here is the gap I found, and it is bigger than I expected.
One note before the data: I am a columnist who reads primary literature, not a clinician. Nothing below tells you what will happen to you specifically. It tells you what happened, on average, to groups of men in controlled trials. Your labs decide your case, not this column.
The number that matters: zero
Here is the figure that reorganized how I read every other timeline claim. In the Testosterone Trials, a coordinated set of placebo-controlled studies in 790 men aged 65 and older with confirmed low testosterone, treatment produced no significant benefit for vitality, measured on a standard fatigue scale [2]. Zero. Not “small.” Not “significant.” Zero, statistically.
That is the exact claim sitting at week one of nearly every timeline I found online: energy comes back first. The best evidence available says otherwise. Meanwhile, the same trial did find significant, measurable improvement in sexual activity, sexual desire, and erectile function, plus a modest bump in mood [2]. So one domain of the promised timeline is real and trial-confirmed. The other, the one everyone leads with, is not.
The comparison nobody runs: what’s confirmed vs. what’s marketed
Laying the trial’s actual findings next to the standard marketing pitch makes the mismatch obvious:
| Claim on the typical timeline chart | What the Testosterone Trials actually found [2] |
|---|---|
| Energy returns fast (often “week one”) | No significant vitality benefit |
| Sexual function improves | Significant improvement, confirmed |
| Mood transforms | Modest improvement, confirmed |
| Precise weekly milestones | Not measured; trials tracked outcomes over the full treatment course, not week-by-week |
Two out of four rows hold up. One is contradicted outright. One was never measured the way it’s presented. That’s a 50 percent accuracy rate on the part of the timeline that’s supposed to set your expectations, and the miss is the headline claim.
The gate before the timeline even starts
Before any of those weeks count, there’s a number that decides whether the whole exercise applies to you at all: two. The Endocrine Society guideline requires symptoms plus unequivocally low testosterone, confirmed on a second fasting morning blood test, not one borderline reading [1]. The FDA’s own labeling backs this up, restricting approved testosterone to hypogonadism from a medical condition, not to low testosterone from aging alone, and stating explicitly that benefit and safety for age-related decline haven’t been established [5].
So the real week zero isn’t a shot. It’s a repeat blood draw. Any chart that opens with an injection has already skipped the step that determines whether the rest of the chart is relevant to you personally.
The percentages the glossy timelines never chart
Two safety numbers matter more than any energy milestone, and both are absent from the marketing versions.
Blood count. Testosterone can raise red blood cell count over time, which is why the Endocrine Society guideline builds a full first-year monitoring cadence, hematocrit, repeat testosterone, and prostate-risk checks, into the treatment itself [1]. That’s a real, recurring timeline. It just doesn’t make for a good chart because “get bloodwork again” isn’t inspiring.
Fertility. Standard testosterone suppresses your own hormone production and can lower sperm count. The alternatives have their own numbers worth comparing. In a randomized trial, enclomiphene matched a testosterone gel for raising testosterone, while also raising LH and FSH and conserving sperm counts [4]. And in a 2025 real-world analysis, HCG lifted the share of androgen-suppressed men with a normal total motile sperm count from 5 percent to 58 percent [6], a 53-point swing, though the paper is clear that not every man got there. Worth flagging since I checked: enclomiphene is not FDA-approved; it’s compounded under prescription, and any provider worth using will say so upfront [5].
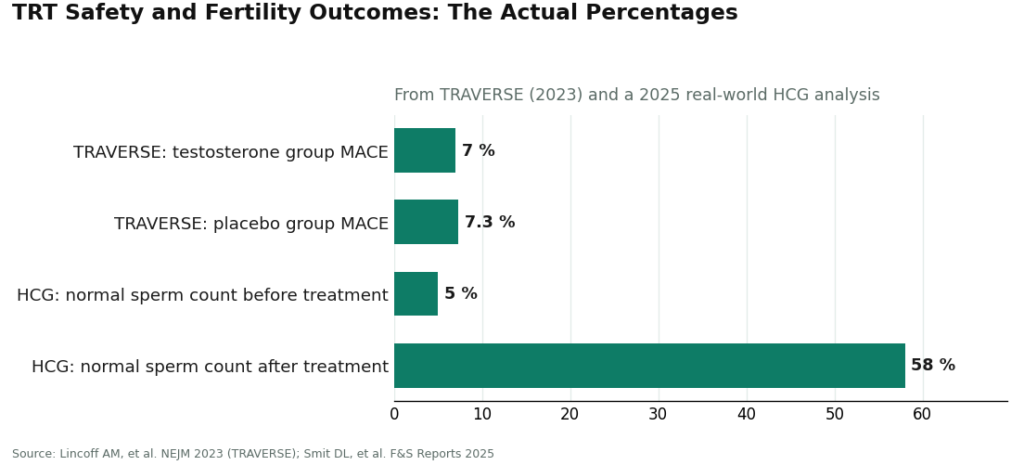
The heart number: 7.0 vs. 7.3
The cardiovascular question used to get a shrug for an answer. TRAVERSE, published in 2023, gave it a real one: 5,246 men aged 45 to 80 with low testosterone and existing or high cardiovascular risk, randomized to testosterone or placebo [3]. The result: major adverse cardiac events in 7.0 percent of the testosterone group versus 7.3 percent on placebo, a difference small enough to call noninferior [3]. The FDA responded by dropping the old boxed cardiovascular warning and adding a new one, for increased blood pressure, instead [5].
Read that gap again: 0.3 percentage points. That’s genuinely reassuring on the specific question of heart attacks and strokes. But the same trial recorded higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group [3]. So “noninferior on MACE” is not the same as “no monitoring needed.” It’s an argument for the boring blood-work schedule above, not a reason to skip it.
My honest timeline, once you strip the marketing
Put the numbers in order and this is what I’d actually trust:
- Two morning blood tests, confirming a genuine deficiency, before anything else [1][5].
- If confirmed, gradual improvement over weeks to months in sexual function and mood, the two domains with trial support [2].
- No promised energy transformation, because the best trial didn’t find one [2].
- Recurring labs through year one and beyond, tracking blood count and other markers [1].
- A fertility conversation up front if it matters to you, with enclomiphene or HCG as documented options, not afterthoughts [4][6].
- Ongoing monitoring for the cardiovascular tradeoffs TRAVERSE actually found, atrial fibrillation, kidney injury, pulmonary embolism, even with reassuring MACE numbers [3].
Six steps, none of them a calendar of feelings, all of them traceable to a citation.
Where supervision actually shows up in the data
Every step above depends on the same unglamorous variable: someone tracking your labs across time instead of you managing a vial alone. FormBlends is one telehealth entity built around that structure. It runs physician-supervised intake, a licensed clinician reviews your profile before anything is prescribed, and any prescription is filled through a licensed 503A compounding pharmacy. I’m citing it once as an example of the supervised-access model this data actually supports, not as a product to buy, and with no promise about how fast you’ll feel anything.
The reason it belongs in a numbers piece is simple: nothing in the trial data above works without repeat testing. A model where a clinician reads your history, labs drive the decisions, a licensed pharmacy fills the order, and follow-up testing drives any dose change, is the only version of “the timeline” the evidence actually backs.
What I’d tell a friend, in figures
If a friend asked, I wouldn’t hand him a chart. I’d hand him four numbers. Two blood tests, minimum, before starting anything. Zero, the vitality benefit the best trial found, so don’t budget your expectations around week-one energy. 0.3 percentage points, the cardiovascular gap TRAVERSE found, reassuring but not a reason to skip monitoring. And 5 to 58, the fertility swing HCG produced in one analysis, worth knowing if that’s on your mind before you start. Everything else is narrative dressed up as data.
Testosterone, enclomiphene, and HCG are prescription treatments. Enclomiphene and any compounded preparation are not FDA-approved finished drug products. Every figure above is a population average from a trial; what shows up on your own bloodwork is a separate, slower question.
Questions I kept getting asked
How long does TRT actually take to work? Weeks to months, for the outcomes the trials actually measured, not a fixed daily schedule. The Testosterone Trials tracked improvements in sexual activity, desire, and erectile function across the full treatment course, not against specific week markers [2]. Track your own progress against your labs and how you feel, not against someone else’s calendar.
Does TRT really boost energy in week one? This is the most inflated claim in circulation. The best available trial found no significant vitality benefit on a standard fatigue scale, even while confirming real gains in sexual function [2]. Some men report feeling more energetic, but the trial-level data doesn’t support banking on it as a reliable early result.
Do I need a blood test before starting? Two, actually. The Endocrine Society guideline requires symptoms plus a confirmed low testosterone reading on a repeat fasting morning test [1], and the FDA limits approved testosterone to hypogonadism from a medical condition rather than aging alone [5]. Skip that step and the rest of the timeline doesn’t apply to you.
Is TRT safe for the heart? TRAVERSE (2023) found testosterone noninferior to placebo for major cardiac events in 5,246 higher-risk men, 7.0 percent versus 7.3 percent, prompting the FDA to remove the old boxed cardiovascular warning [3][5]. That’s a good number. But the same trial found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism on testosterone [3], which is why monitoring continues rather than stopping.
Will TRT affect my fertility, and what are the alternatives? Standard testosterone can suppress your own production and lower sperm count over time. In a randomized trial, enclomiphene matched a testosterone gel on raising testosterone while conserving sperm counts and raising LH and FSH [4]. A 2025 real-world analysis found HCG raised the share of men reaching a normal total motile sperm count from 5 percent to 58 percent [6]. Enclomiphene isn’t FDA-approved and is compounded under prescription, so a legitimate provider will tell you that directly [5].
Verified citations
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Snyder PJ, et al. Effects of Testosterone Treatment in Older Men (The Testosterone Trials). N Engl J Med. 2016. In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Lincoff AM, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023. In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism.
- Wiehle RD, et al. Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Fertil Steril. 2014. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. U.S. Food and Drug Administration. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added.
- Smit DL, et al. Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. F&S Reports. 2025. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment.
Are TRT clinics actually legitimate, or are most of them just pill mills?
Most clinics running through licensed physicians who order labs, review history, and follow up regularly are legitimate medical practices. The ones skipping baseline bloodwork, pushing a purchase before a diagnosis, or offering zero ongoing monitoring are the ones to avoid. Legitimacy is a process question, not a branding question. If a clinic can’t tell you who supervises your care and how often, you have your answer.
How much does TRT through a clinic actually cost per month?
The range runs roughly $100 to $400 per month, depending on the protocol, delivery method, and whether labs and consults get billed separately. Injectable testosterone tends to sit at the lower end; pellets and certain creams push the number up. Most clinics don’t bill insurance for the hormone itself, though some labs might be covered. Get an itemized quote before you sign anything.
Which type of TRT clinic is actually best for long-term care?
The setup that holds up best over time pairs a physician (in-person or telehealth) with a licensed compounding pharmacy, so your protocol can flex with your labs instead of locking you into one fixed dose. Some men find physician-supervised compounding routes, including FormBlends, offer more room to adjust than retail-product-only clinics. The variable that actually matters is whether someone is reading your follow-up labs and changing anything based on them.
Where do you even start looking for a TRT clinic worth trusting?
Start with your primary care doctor or a urologist; a referral builds in a baseline of accountability. Going direct to a clinic instead, verify three things: the prescribing provider holds a current state medical license, the pharmacy filling prescriptions is accredited, and the intake process requires bloodwork before any prescription is written. State medical board sites let you check licenses for free, and that five-minute check tells you most of what you need.
Written by Sena Ellison, reporter. Checking each figure against the cited source. Last reviewed February 2026.
Not professional medical advice. Speak with your healthcare provider before making a change.